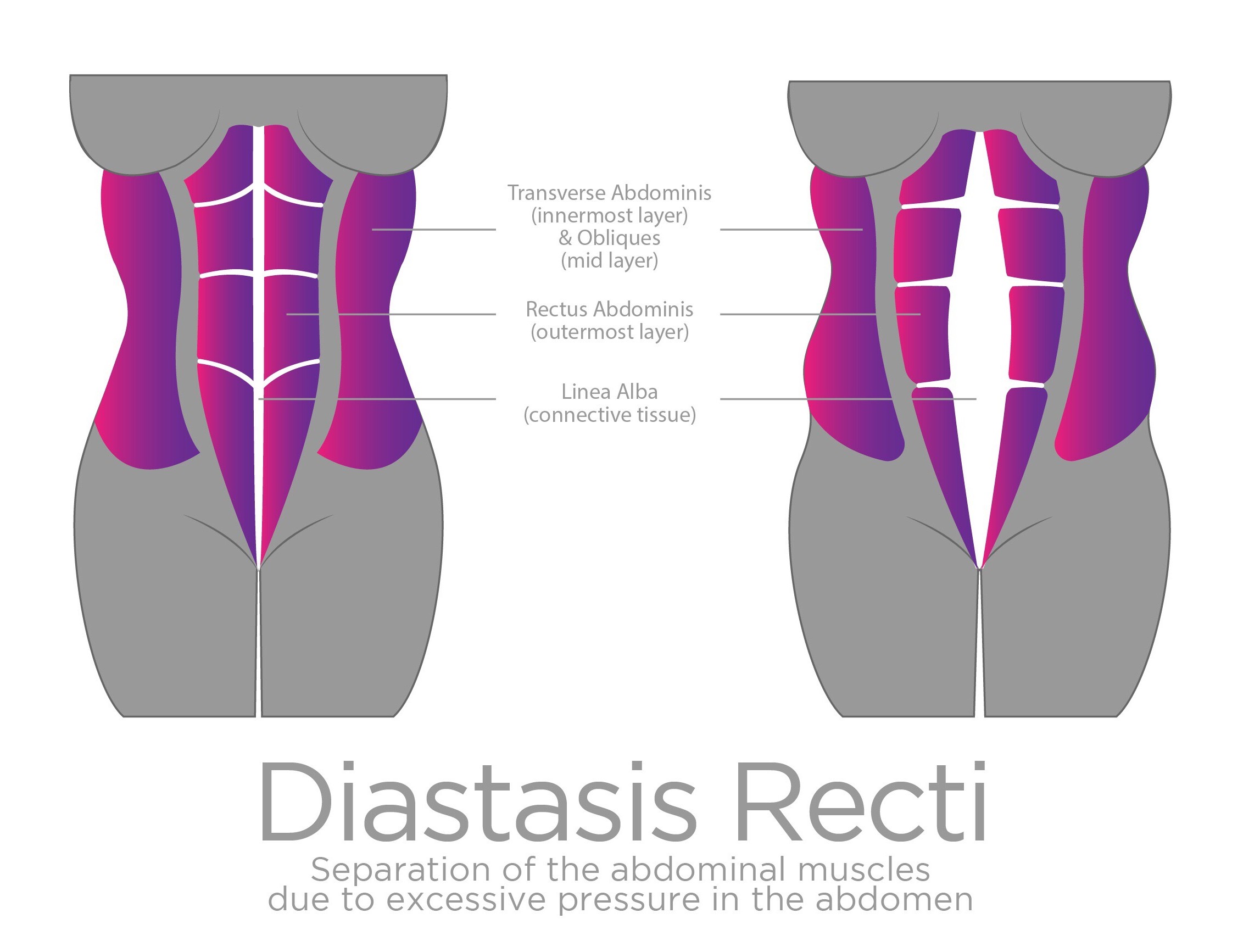
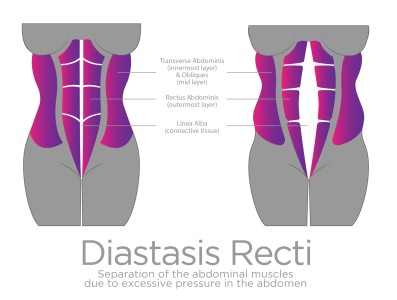
Pregnancy-Related Diastasis Rectus Abdominis (DRA): Top Five Updated Insights!
The discussion points in this blog are based on the findings of a recent Canadian study co-lead by Dr. Sinéad Dufour (McMaster Univeristy, Ontario) and Stéphanie Bernard (Laval University, Quebec).
1) Determining the “gap” between the rectus abdominis muscles is not clinically relevant. Our experts agreed (over 80% consensus) that determination of the inter-recti distance (IRD), the conventional method of actually determining the presence of DRA, is not clinically relevant. Rather our experts contend that like dynamic tissues elsewhere in the body, meaningful assessment techniques need to garner aspects of the tissue function and behaviour. So, if determining IRD was not recommended by our experts, what is? Assessing for the development of tension through the linea alba during a voluntary pelvic floor contraction topped the list at almost 90% consensus.
Summary 1: Don’t get too obsessed about how many fingers you can fit inside the “gap”. The tension of your abdominal wall is what matters more!
2) The function of the linea alba is interdependent with the function of the pelvic floor. As demonstrated in insight number one, our experts indicate a clear connection between the function of the linea and alba and the pelvic floor. Beyond assessment, this understood interdependence was highlighted in many of the other practice principles that were generated. For example, one practice principle highlighting this was applied to all three domains of perinatal care indicated the following: Commence inner unit exercises that facilitate optimal isolated and synergistic activation of the inner unit and once control achieved, progress with tailored outer unit and functionally oriented exercises.
Summary 2: Your pelvic floor and abdominal muscles work together! You need to ensure you know how to properly engage your pelvic floor muscles (aka kegels) to activate your core!

3) Optimal Management of intra-abdominal pressure is key.
Moving from the inner unit muscles to the concept of the canister these muscles actually create, of which the lina alba is anatomically and functionally a part of, is what we call the “manometric pressure system”. Our experts were clear in their agreement that DRA, as understood to be more than just widened IRD, needs to be considered within the context of the
manometric pressure system. The general summary statement that was developed conveys this important perspective and is outlined at the end of the article 1 Establishing best practice principles for pregnancy-related diastasis rectus abdominis: A consensus study. Presentations: ICS, Florence Italy; CSM, New Orleans. Manuscript in development.
Summary 3: Diastasis Recti is caused by excessive pressure pushing out on the abdominal wall (think growing baby, poor posture or breathing mechanics, even a man with a beer belly can get diastasis recti). It’s not as simple as just calling the condition “separated abs”.
4) Women’s health physiotherapists have an importance advocacy role with respect to optimizing pelvic and abdominal health through labour and delivery. Although it was not until round 2 of the Delphi consensus that this insight was transpired, by
the end of round 3, four practice principles were established within the domain of intra-partum care. The two practice principles that were considered to be of primary importance in this domain were: Advocating for the ability to be mobile during labour and avoiding directed pushing practices that increase intra-abdominal pressure for sustained periods and close the
glottis (Eg. Valsalva manoeuver). It is exciting and important that our experts acknowledge important emerging roles for physiotherapists that promote women’s pelvic and abdominal health upstream!
Summary 4: To reduce unnecessary strain on the pelvic floor and abdominal wall, research shows that women should be allowed to be mobile during labour and not confined to a bed. They should also avoid intense valsalva bearing down style pushing, and ideally wait until they feel the urge to push themselves.
5) There is no place to recommendations that could potentially induce fear of movement.
Our Delphi consensus commenced with 82 statements and ended with 28 developed practice principles after three rounds of iteration. The language in all 28 final practice principles was tweaked and modified through each stage based on experts’ feedback to ensure that potential fear of movement would not be elicited. As one of the lead researchers on this work I was happy but not surprised that our expert colleagues hold this important and scientifically substantiated perspective. Other recent research of mine on the topic of pregnancy-related pelvic girdle pain confirmed that pelvic health physiotherapists do a much better job of using language that will not elicit fear when compared to physiotherapists who do not have additional post-graduate pelvic health training.
Summary 5: Don’t be afraid to move! Movement is medicine. Find yourself a specialized pelvic physiotherapist to help you if you’re experiencing pelvic pain!
To close, I leave you with a summary statement from this work that puts it all together. Pregnancy-related DRA represents an important and under-recognized concern. All relevant health and fitness providers working with pregnant women should know how to promote best care practices for this condition, however general agreement of what constitutes the best approach to is lacking. Given that the complex three-dimensional tissue of the linea alba is intrinsic to the thoraco-pelvic abdominal manometric system, compromised integrity of the linea alba needs to be considered within the context of this system. As experts in women’s health, we have come to understand that the impairments and dysfunctions related to DRA as multi-dimensional and multifactorial. Further, in line with other thoracic, lumbar and pelvic conditions we manage in the profession of physiotherapy, the interaction between the musculoskeletal, nervous and immune systems represents a central aspect of our global care approach, which is then individually tailored. Thus, our approach allows for the integrated targeting of modifiable factors that are potential drivers of DRA and associated impairments or participation restrictions across multiple dimensions. As a group we have agreed that a set of practice principles are needed when working with women in order to guide clinical decision making with respect to pregnancy-related DRA. These practice principles have been developed with intent of guiding practice of all relevant care providers.